


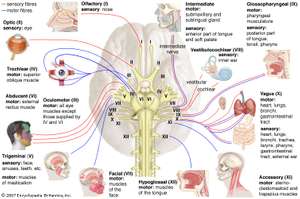
Cranial nerve testing is BORING!
In entry-level physical therapy education, I remember learning (well, memorizing at the time) the cranial nerves. We did everything we could to remember it including the most entertaining mnemonics :)
It never "stuck" with me to include this in daily clinical practice examination until I followed through with my Fellowship Program and specifically used it in a manner to rule-out conditions, specific conditions at that.
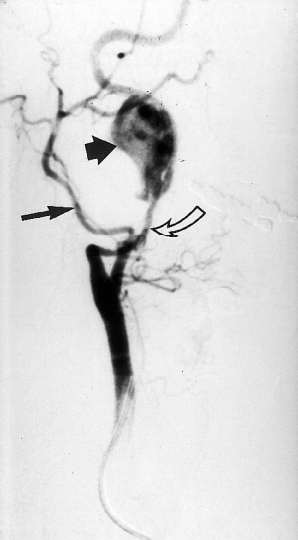
Table from Muhammed et al 2019 Post-treatment NDI was significantly lower in Group C compared to the other two groups (p<0.001) and was comparable in groups A and B (p=1.000). The percentage drop of NDI was significantly higher in Group C compared to the other two groups (p<0.874), but the magnitude of NDI drop was comparable between Groups A and B (p=1.000, Table 2).
I enjoyed reading an article entitled, "Extracranial internal carotid artery aneurysm presenting as symptomatic hypoglossal and glossopharyngeal nerve paralysis" in The Journal of Laryngology & Otology in 2004. Even though "old" in today's standards for evidence-based practice, I want to point out the concepts that arise from the clinical reasoning and its relationship to Cranial Nerves and the Internal Carotid Artery.
One concept I always push in our Cervicogenic Dizziness Course is that we need to be vigilant on the entire cervical vascular system and not just screening for Vertebrobasilar Insufficiency. This ultimately means we need to know about signs/symptoms and clinical characteristics of disorders to the Internal Carotid Artery. We can therefore, make sure we rule-out other sinister conditions to then aid in ruling-in Cervicogenic Dizziness as the diagnosis.
Cervicogenic Dizziness Course
Just as described in our Optimal Sequence Algorithm, the first step prior to even assessing the vascular system, especially any mechanical disruption, is to go "back to basics".
This involves initially examining the cranial nerves, especially the ones that may be affected first in a patient presenting with internal carotid artery dysfunction.

Cervicogenic Dizziness Course
A negative finding on cranial nerve examination is one of the presenting clinical findings that led the team in this paper to perform an ultrasound on the neck and then refer for MR imaging.
You may ask what led to performing cranial nerve exam. Here you go:
Are your dizzy and neck patients getting stuck at being 75% better? We can help.
Here are the paper highlights:
SUBJECTIVE
- After a patient went to chiropractor for 3 visits 1 month prior, she self-admitted to ENT office for painful swelling in jaw .
- She had several bouts of dizziness associated with turning her head to her left.
- She had bouts of light-headiness.
- She also developed loss of hearing in her left ear.
Objective
- Odd sensation with swallowing
- Marked tongue deviation to the right side with tongue protrusion
Cervicogenic Dizziness Course
So how does this relate to Cervicogenic Dizziness?
- The subjective findings above could mean mechanical or non-mechanical source of symptoms but objective findings indicate a cranial nerve palsy response to cranial nerve testing (specifically hypoglossal and glossopharyngeal).
- Patient could have self-admitted to a physical therapy office instead of ENT, so ultimately we need to be able to fully examine someone with initial thoughts of non-mechanical symptoms unless proven otherwise.
- Positional dizziness, such as turning head to the left, are typical symptoms associated with the diagnosis of Cervicogenic Dizziness.
- Lightheadiness is a typical symptom associated with the diagnosis of Cervicogenic Dizziness.
- She had a recent minor trauma, which in this case, was a trip to the chiropractor with assumption of a manipulation performed.
- Instead of seeing another clinician, she could have simply had a recent minor trauma from looking up, played golf, or even had a concussion or in a car accident.
Nevertheless, we recommend clinicians screen appropriately with subjective and objective examination procedures, especially if someone is presenting with symptoms of lightheadiness, dizziness and/or vertigo.
Cervicogenic Dizziness Course
You can learn more about the screening and treatment process of Cervicogenic Dizzinesss through Integrative Clinical Concepts, where the authors (husband–a manual therapist a wife—a vestibular specialist), teach a very unique course combining both the theory and practice of vestibular and manual principles in their 2-day course. Pertinent to this blog post, the 2nd day includes the “Physio Blend”, a multi-faceted physiotherapist approach to the management of Cervicogenic Dizziness, which includes treatments of the articular and non-articular system of manual therapy and the most updated sensorimotor exercise regimen.
If you would like to host a course for your staff (either a vestibular, neuro, sports or ortho clinic), please do not hesitate to contact me at harrisonvaughanpt@gmail.com for more information.
AUTHORS
Harrison N. Vaughan, PT, DPT, OCS, Dip. Osteopracic, FAAOMPT
Instructor: Cervicogenic Dizziness for Integrative Clinical Concepts
Danielle N. Vaughan, PT, DPT, Vestibular Specialist
Instructor: Cervicogenic Dizziness for Integrative Clinical Concepts